Lyme Disease in Tennessee May Be Underreported
Studies suggest Lyme disease cases in Tennessee may be underreported.
Insurance data identified far more cases than state surveillance records.
Clinical diagnosis often differs from public health reporting criteria.
Lyme disease Tennessee underreporting may be significant, with studies suggesting cases are far higher than official surveillance data.
Researchers examining insurance claims and public health records identified major gaps in reported Lyme disease cases in Tennessee.
A study using data from BlueCross BlueShield of Tennessee (BCBST) and the Center for Environmental and Communicable Diseases found approximately 196 unreported cases per year.
Cases Far Exceed Official Reports
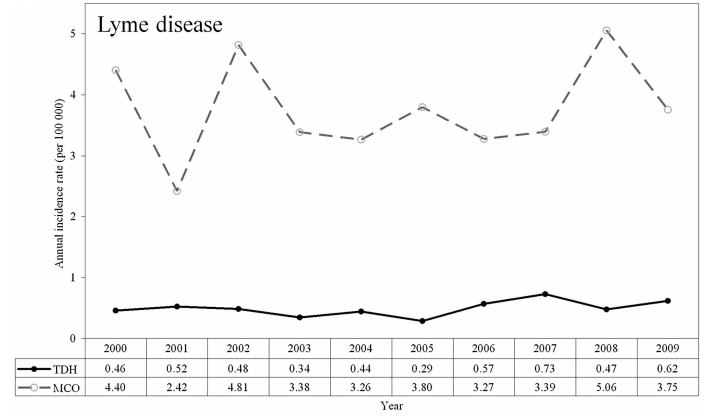
In a follow-up analysis, the incidence of Lyme disease in Tennessee was found to be 19 times higher than that reported by the Tennessee Department of Health (TDH).
Between January 2011 and June 2013:
- 1,367 cases were identified in the BCBST database
- Only 74 cases were reported by the TDH
This discrepancy highlights substantial underreporting in official surveillance systems.
Patients searching for “How common is Lyme disease in Tennessee?” may not realize surveillance reports can underestimate clinically diagnosed cases.
Limitations of Surveillance Criteria
Less than 4% of patients in the BCBST database met the national surveillance case definition for Lyme disease.
The surveillance definition requires:
- Clinical evidence (erythema migrans rash or late manifestations)
- Laboratory confirmation (two-tier testing)
- Documented exposure in an endemic area
Many clinically diagnosed cases do not meet these strict criteria, despite evidence of illness.
Clinical Diagnosis vs Surveillance Reporting
Approximately 50% of patients in the BCBST database had a documented history of Lyme disease.
For an additional 25% of patients, there was insufficient information to confirm prior diagnosis.
Most Lyme disease diagnoses are made based on clinical judgment rather than strict surveillance criteria.
This distinction is important because surveillance definitions are designed for public health tracking—not for individual patient diagnosis and treatment decisions.
Why This Matters
The study suggests that hundreds of Lyme disease cases may be missing from official surveillance systems.
Despite these findings, the authors did not recommend incorporating administrative claims data into the Tennessee Department of Health reporting system.
This gap raises important questions about how Lyme disease is tracked—and whether current systems accurately reflect the true burden of illness.
Clinical Perspective
Lyme disease surveillance systems are designed for public health tracking, not for clinical diagnosis.
Clinicians should rely on clinical judgment when evaluating patients, particularly in regions where Lyme disease may be underrecognized.
Tennessee clinicians evaluating tick-borne diseases may encounter Lyme disease even in areas considered lower incidence regions.
Improving surveillance methods may be essential to better understand the true scope of Lyme disease.
For additional discussion on delayed diagnosis and recognition challenges, see Delayed Lyme disease diagnosis and Lyme test accuracy.
Frequently Asked Questions
Is there Lyme disease in Tennessee?
Yes. Published studies and insurance claims data suggest Lyme disease occurs in Tennessee more often than official reports may indicate.
Why might Lyme disease be underreported in Tennessee?
Strict surveillance criteria may exclude clinically diagnosed cases that do not meet laboratory or reporting requirements.
Does a surveillance definition determine clinical diagnosis?
No. Surveillance definitions are designed for public health reporting and may not reflect all clinically diagnosed cases.
References:
- Jones SG et al. J Am Med Inform Assoc. 2012.
- Enhancing Lyme Disease Surveillance Using Administrative Claims Data.
Dr. Daniel Cameron, MD, MPH
Lyme disease clinician with over 30 years of experience and past president of ILADS.
Symptoms • Testing • Coinfections • Recovery • Pediatric • Prevention