Borrelia Persister Cells and Persistent Lyme Disease
Borrelia persister cells may survive antibiotic exposure
Slow-growing bacterial forms may contribute to persistent symptoms
Researchers continue to study antibiotic tolerance in Lyme disease
Persistent infection of Borrelia burgdorferi (Bb) has been proven experimentally in Peromyscus mice, laboratory mice, rats, hamsters, gerbils, guinea pigs, dogs and non-human primates. [1-8] Some researchers and clinicians argue that persistent Bb infection may help explain why some Lyme disease patients remain ill after treatment.
According to one study, as many as one-third of patients treated for Lyme disease remain chronically ill. [9]
Learn more about persistent Lyme disease and ongoing symptom mechanisms.
What are Borrelia persister cells?
In a review published in the Bosnian Journal of Basic Medical Sciences, Dr. Emir Hodzic explored the role persister cells may play in chronic Lyme symptoms. [10]
“The main culprit responsible for the tolerance of pathogens to antibiotics is a specialized survivor – a persister,” states Hodzic. [10]
Persister cells are dormant or slowly dividing bacterial forms that may survive exposure to antimicrobial therapy. Because many antibiotics target actively dividing bacteria, dormant organisms may be more difficult to eradicate.
Unlike classic antibiotic resistance, persister cells are thought to represent antibiotic tolerance rather than permanent genetic resistance.
Persister forms may emerge over time
During infection, Borrelia burgdorferi may generate weakened or attenuated spirochetes that divide more slowly due to plasmid loss. Researchers suggest these altered bacterial forms may become less susceptible to antimicrobial killing.
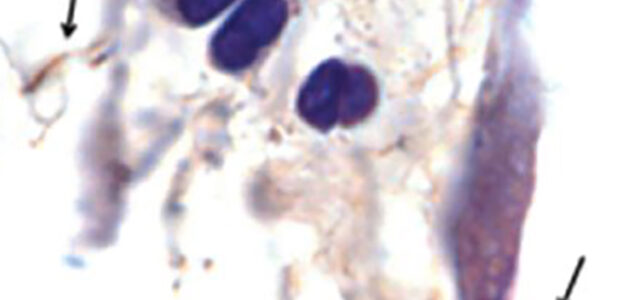
Researchers identified spirochetes within mouse tissue 12 months after antibiotic treatment, supporting ongoing investigation into Borrelia persistence following therapy.
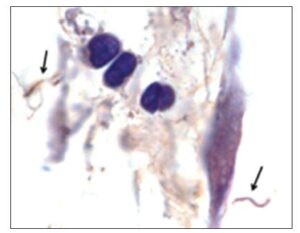
According to Hodzic, “There is clear scientific evidence that a small, heterogeneous subpopulation of surviving spirochetes shows tolerance to antimicrobial agents and can persist in a host for a prolonged period following therapy.” [10]
In one mouse study, non-cultivable spirochetes reappeared in tissues 12 months after antibiotic treatment.
The authors proposed that plasmid loss may partly explain why antibiotic treatment appears more effective during early infection than later stages of disease.
Antibiotic tolerance versus antibiotic resistance
The discussion surrounding Borrelia persister cells is often misunderstood.
Persister mechanisms are generally described as antibiotic tolerance rather than classic antibiotic resistance.
Hodzic explains that tolerance occurs when antibiotics fail to eliminate slowly dividing or dormant bacterial subpopulations despite adequate exposure to antimicrobial therapy.
This differs from classic resistance mechanisms where bacteria genetically acquire the ability to grow despite antibiotics.
Learn more about Lyme disease treatment approaches and challenges involving persistent symptoms.
Researchers continue studying persistent Lyme mechanisms
Researchers continue investigating several possible mechanisms contributing to persistent Lyme symptoms, including:
- Persistent infection
- Immune dysregulation
- Inflammation
- Biofilm formation
- Small fiber neuropathy
- Autonomic dysfunction
The exact role of persister cells in human disease remains an active area of investigation.
Studies involving animal models, microbial tolerance, and persistent bacterial forms continue to shape ongoing discussions surrounding chronic Lyme disease and PTLDS.
Clinical Perspective
Borrelia persister cells remain one of the more controversial and actively debated topics in Lyme disease research.
While experimental evidence supports the existence of antibiotic-tolerant Borrelia forms in animal models, researchers continue to debate how these findings apply to persistent symptoms in human illness.
The growing literature surrounding microbial persistence highlights the complexity of Lyme disease biology and the need for continued investigation into mechanisms underlying chronic symptom burden.
Frequently Asked Questions
What are Borrelia persister cells?
Persister cells are dormant or slow-growing bacterial forms that may survive antibiotic exposure despite not having classic genetic antibiotic resistance.
Are persister cells the same as antibiotic resistance?
No. Persister cells are generally considered a form of antibiotic tolerance rather than permanent antibiotic resistance.
Can Borrelia persister cells cause chronic Lyme disease?
Researchers continue studying whether persister cells contribute to persistent symptoms in some Lyme disease patients.
Have persister cells been demonstrated experimentally?
Yes. Studies in animal models have demonstrated persistent Borrelia organisms following antibiotic treatment.
Why are persister cells difficult to treat?
Many antibiotics target actively dividing bacteria, while persister cells may remain dormant or divide very slowly.
Clinical Takeaway
Borrelia persister cells and antibiotic tolerance remain important areas of Lyme disease research.
Although the exact clinical significance in human illness remains under investigation, studies involving persistent bacterial forms continue to influence discussions surrounding chronic symptoms, treatment response, and recovery in Lyme disease.
Understanding microbial persistence may help clarify why some patients continue to experience symptoms despite standard antibiotic therapy.
Related Articles
These related articles explore neurologic Lyme disease, delayed diagnosis, persistent symptoms, and recovery challenges associated with chronic Lyme illness.
Neurologic Lyme Disease
Post-Treatment Lyme Disease Syndrome
Delayed Lyme Disease Diagnosis
Recovery From Lyme Disease
Lyme Disease Misdiagnosis
References
- Schwan TG, Burgdorfer W, Schrumpf ME, Karstens RH. The urinary bladder, a consistent source of Borrelia burgdorferi in experimentally infected white-footed mice (Peromyscus leucopus). J Clin Microbiol. 1988;26(5):893-895.
- Barthold SW, de Souza MS, Janotka JL, Smith AL, Persing DH. Chronic Lyme borreliosis in the laboratory mouse. Am J Pathol. 1993;143(3):959-971.
- Moody KD, Barthold SW, Terwilliger GA, Beck DS, Hansen GM, Jacoby RO. Experimental chronic Lyme borreliosis in Lewis rats. Am J Trop Med Hyg. 1990;42(2):165-174.
- Goodman JL, Jurkovich P, Kodner C, Johnson RC. Persistent infection after antibiotic therapy in hamster model of Lyme disease. J Clin Microbiol. 1991;29(5):894-896.
- Preac-Mursic V, Patsouris E, Wilske B, Reinhardt S, Gross B, Mehraein P. Persistence of Borrelia burgdorferi in experimentally infected animals after antibiotic treatment. Infection. 1990;18(6):332-341.
- Sonnesyn SW, Manivel JC, Johnson RC, Goodman JL. A guinea pig model for Lyme disease. Infect Immun. 1993;61(11):4777-4784.
- Straubinger RK, Summers BA, Chang YF, Appel MJ. Persistence of Borrelia burgdorferi in experimentally infected dogs after antibiotic treatment. J Clin Microbiol. 1997;35(1):111-116.
- Roberts ED, Bohm RP Jr, Cogswell FB, et al. Chronic Lyme disease in the rhesus monkey. Lab Invest. 1995;72(2):146-160.
- Cameron DJ, Johnson LB, Maloney EL. Evidence assessments and guideline recommendations in Lyme disease: the clinical management of known tick bites, erythema migrans rashes and persistent disease. Expert Rev Anti Infect Ther. 2014;12(9):1103-1135.
- Hodzic E. Lyme borreliosis: Is there a preexisting variation in antimicrobial susceptibility among Borrelia burgdorferi strains? Bosn J Basic Med Sci. 2015;15(3):1-13.
- Embers ME, Barthold SW, Borda JT, et al. Persistence of Borrelia burgdorferi in rhesus macaques following antibiotic treatment of disseminated infection. PLoS One. 2012;7(1):e29914.
- Cabello FC, Godfrey HP, Newman SA. Hidden in plain sight: Borrelia burgdorferi and the extracellular matrix. Front Cell Infect Microbiol. 2022;12:1036483.
Dr. Daniel Cameron, MD, MPH
Lyme disease clinician with over 30 years of experience and past president of ILADS.
Symptoms • Testing • Coinfections • Recovery • Pediatric • Prevention

