Lyme Babesia Coinfection: When One Diagnosis Hides Another
Lyme Babesia coinfection is more common than many realize—and in some cases, Lyme disease is the diagnosis that gets missed. In this case report, an elderly man diagnosed with Babesia nearly had his Lyme disease overlooked until he developed Bell’s palsy. :contentReference[oaicite:0]{index=0}
The importance of clinicians considering other tick-borne diseases, such as Babesia, when evaluating patients with Lyme disease has been addressed in the literature. Surprisingly, however, physicians may not consider Borrelia burgdorferi as a coinfection in patients already diagnosed with another tick-borne illness.
Such was the case for an elderly man diagnosed with Babesia, whose Lyme disease was nearly overlooked, according to a case report by Zaiem and colleagues.
Why Lyme Disease Gets Overlooked
This case highlights an important clinical gap: once one tick-borne disease is identified, clinicians may not consider additional infections.
For years, Lyme disease has been overlooked as a possible cause behind patients’ symptoms.
One study by Dr. Brian Fallon and colleagues found Lyme disease was overlooked an average of 2 years in patients later diagnosed with Lyme encephalopathy, including individuals initially thought to have psychiatric illness.
These patients were initially diagnosed with conditions such as paranoia, dementia, schizophrenia, bipolar disorder, panic attacks, major depression, anorexia nervosa, and obsessive-compulsive disorder.
According to a case series by Dr. Daniel Cameron, Lyme disease was overlooked for years in some patients before diagnosis was confirmed with positive IgG Western blot bands.
Treatment Delays Lead to Poor Outcomes
Delays in diagnosis and treatment can have serious consequences.
In Fallon’s study, Lyme encephalopathy patients—whose diagnosis was delayed by an average of two years—remained ill for an average of nine years after onset.
In the Cameron case series, patients with delayed treatment were six times more likely to fail their initial course of treatment compared to those treated within 30 days.
Case Report: Lyme Babesia Coinfection Almost Missed
“Co-infection with Borrelia should be considered in patients with atypical presentation or with a poor response to proper therapy,” concludes Zaiem.
A case report published in QJM: An International Journal of Medicine describes a 70-year-old man presenting with headaches, high fevers, vomiting, and decreased urine output.
Babesia was suspected based on his residence in Eastern Long Island, NY, and malaria was also considered due to recent travel history.
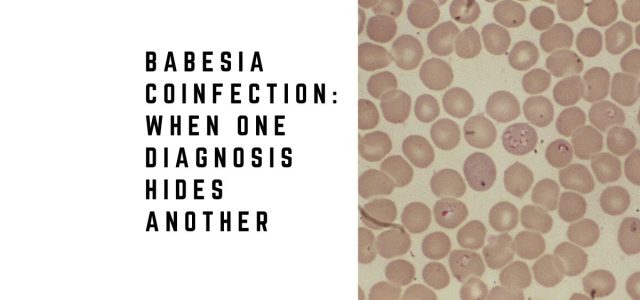
Laboratory testing supported the Babesia diagnosis. Peripheral blood smear revealed intracellular rings consistent with B. microti, and PCR confirmed infection.
The patient improved with treatment including doxycycline and quinine.
However, just prior to discharge, he developed Bell’s palsy. Subsequent testing confirmed Lyme disease.
Without the development of Bell’s palsy—seen in only 9% of Lyme cases—the Lyme infection may have remained undiagnosed.
Lyme Babesia Coinfection Increases Severity
Tick-borne diseases are often complex, particularly when multiple infections are present.
Studies show that ticks frequently carry more than one pathogen. In one study from upstate New York:
- 55% carried Borrelia burgdorferi
- 18.2% carried Anaplasma phagocytophilum
- 3.2% carried Babesia microti
- 1.5% carried Ehrlichia chaffeensis
Krause and colleagues found that patients with both Babesia and Lyme disease experience more severe illness and longer symptom duration.
Steere and colleagues similarly reported increased symptom burden—including fevers and chills—in coinfected patients.
Co-infections Affect Treatment Outcomes
Coinfections can significantly affect treatment response.
Krause concluded that clinicians should test for Babesia and other infections in Lyme disease patients with prolonged flu-like illness who do not respond to appropriate therapy.
Poor outcomes—including transverse myelitis and fatal pancarditis—have been reported in patients with combined infections.
Zaiem and colleagues emphasize:
“When patients present with malaria-like illness in endemic areas, physicians should consider Babesia—and also evaluate for Borrelia coinfection in cases with atypical presentation or poor response to treatment.”
Clinical Takeaway
Lyme Babesia coinfection is frequently missed—and delayed diagnosis can significantly worsen outcomes. Key diagnostic considerations:
- Consider Lyme disease in patients with documented tick-borne illness and atypical symptoms or poor response to therapy
- Bell’s palsy or neurologic findings may reveal missed Lyme coinfection
- Diagnostic delays average 2 years in some patients and increase treatment failure risk sixfold
- Coinfection increases disease severity, symptom burden, and complication risk
- Ticks commonly carry multiple pathogens, making coinfection evaluation essential
Frequently Asked Questions
Can you have Babesia without Lyme disease?
Yes. Babesia can occur alone, but clinicians should test for Lyme disease when symptoms are atypical or treatment response is poor.
Why do doctors miss Lyme disease in Babesia patients?
Once one infection is identified, additional infections may not be considered. Lyme disease may also be misdiagnosed as psychiatric illness.
How does coinfection affect treatment outcomes?
Coinfected patients often experience more severe illness, longer duration, and higher complication rates.
What should I do if Babesia treatment isn’t working?
Discuss additional testing for Lyme disease and other coinfections with your physician.
For comprehensive Babesia information organized by topic—including symptoms, testing, and treatment—visit our complete Babesia guide.
Related Reading
- Babesia and Lyme: What Patients Need to Know
- Lyme Disease Co-Infections
- When Lyme Treatment Fails: Could It Be Babesia?
References
- Zaiem F et al. QJM. 2015.
- Fallon BA et al. Neurology. 2008.
- Cameron DJ. J Eval Clin Pract. 2007.
- Krause PJ et al. JAMA. 1996.
- Aliota MT et al. Vector Borne Zoonotic Dis. 2014.
Dr. Daniel Cameron, MD, MPH
Lyme disease clinician with over 30 years of experience and past president of ILADS.
Symptoms • Testing • Coinfections • Recovery • Pediatric • Prevention


