STARI vs Lyme Disease: How to Tell the Difference After a Tick Bite
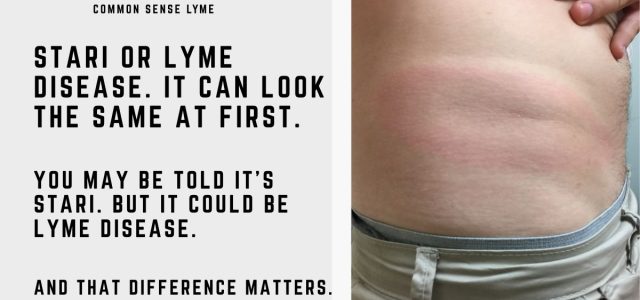
STARI vs Lyme disease can be difficult to distinguish after a tick bite. Both conditions may cause an erythema migrans–type rash, fatigue, fever, headache, and muscle aches.
This overlap can delay diagnosis and treatment—especially when physicians assume Lyme disease is uncommon in certain regions.
In clinical practice, I have seen patients in the southern United States diagnosed with STARI who were not informed that Lyme disease could still be a possibility.
As tick populations expand and overlap geographically, relying on location alone can lead to missed or delayed diagnosis. A Lyme-like rash in the South does not always exclude Lyme disease.
In their article
“Southern Tick-Associated Rash Illness: Florida’s Lyme Disease”
, Abdelmaseih and colleagues describe a patient case highlighting the similarities and differences between STARI and Lyme disease.1
Case Presentation
The patient was bitten by a lone-star tick on her right leg while camping in Gainesville, Florida. After removing the tick, she noticed a pruritic target-like erythematous lesion.
Two weeks later she developed persistent fever, headache, and diffuse myalgias for four days following the tick bite.
On presentation she had:
- Fever of 100.5°F
- Tachycardia of 127 BPM
- Low white blood cell count
- Anemia
- Thrombocytopenia
- Elevated liver function tests
Fortunately, the patient’s symptoms resolved with a 14-day course of doxycycline.
STARI and Lyme Disease: Similarities and Differences
The authors discussed several similarities between STARI and Lyme disease.
“The associated rash is similar if not indistinguishable from Lyme disease erythema migrans, with lymphocytic dermal infiltrate.”
Both STARI and Lyme disease diagnoses rely heavily on clinical judgment.
“At the present time there is no approved diagnostic modality to identify STARI; therefore diagnosis must rely on clinical evidence including erythema migrans and tick exposure.”
This creates an important challenge:
Patients may be diagnosed based largely on geography rather than definitive testing.
Geographic Clues Are Becoming Less Reliable
The diagnosis of STARI and Lyme disease has traditionally relied on geographic exposure.
“Diagnosis usually relies on geographic association (STARI from central Texas and Oklahoma eastward across the southern states and along the Atlantic coast as far north as Maine, versus Lyme disease in the Northeast, Mid-Atlantic, and Upper Midwest).”
But these geographic assumptions are becoming less dependable as tick populations expand.
Lone-star ticks are increasingly found outside traditional southern regions, while black-legged ticks continue spreading into new areas of the South.
Tick distribution maps are changing faster than many diagnostic assumptions.
Could Lyme Disease Be Overlooked?
One concern is whether some patients labeled with STARI may actually have Lyme disease or another tick-borne illness.
Unlike Lyme disease, STARI still lacks:
- A confirmed causative organism
- Standardized diagnostic testing
- Long-term outcome data
- Established treatment guidelines
It has often been assumed that STARI does not cause long-term complications. However, much about the illness remains unknown.
“A recent study has suggested that STARI is transmitted by the lone-star tick Amblyomma americanum; however, much is still unknown about STARI.”
This uncertainty becomes especially important when patients continue experiencing fatigue, neurologic symptoms, or persistent pain after treatment.
Treatment Questions Remain
The treatment of STARI is also uncertain.
“STARI is often treated as Lyme disease with doxycycline twice daily for 14 days; however, there is no approved treatment yet.”
Clinically, many physicians treat STARI similarly to early Lyme disease because distinguishing the two conditions with certainty may be difficult.
The consequences of overlooking Lyme disease—or co-infections such as Babesia or Anaplasmosis—can be significant.
Why This Matters Clinically
The debate surrounding STARI highlights a broader issue in tick-borne illness:
Many diagnoses still rely heavily on pattern recognition rather than definitive laboratory confirmation.
Patients with Lyme-like symptoms should be evaluated carefully—even when they live outside traditional “Lyme-endemic” regions.
This is particularly important when symptoms evolve, persist, or involve neurologic, cardiac, or autonomic dysfunction.
Learn more about delayed Lyme disease diagnosis.
Questions Addressed in This Podcast
- What is STARI?
- Are there differences between STARI and Lyme disease rashes?
- Are there differences in the ticks responsible for infection?
- How is STARI diagnosed compared with Lyme disease?
- What clinical evidence is needed to diagnose STARI?
- What are the consequences if Lyme disease or co-infections are overlooked?
- What do we know about ticks in the southern United States?
WATCH PODCAST BELOW
CLICK BELOW TO LISTEN TO PODCAST
Frequently Asked Questions
What is STARI?
STARI (Southern Tick-Associated Rash Illness) is a Lyme-like illness associated with the lone-star tick that can produce an erythema migrans–type rash.
How is STARI different from Lyme disease?
STARI and Lyme disease share similar symptoms and rashes but are associated with different tick species and may involve different underlying infections.
How is STARI diagnosed?
There is no approved laboratory test for STARI. Diagnosis is based primarily on clinical findings and tick exposure history.
How is STARI treated?
STARI is commonly treated with doxycycline, although no standardized treatment guidelines currently exist.
Can Lyme disease occur in the South?
Yes. Lyme disease can occur in southern states, and geographic assumptions alone should not exclude the diagnosis.
References:
- Abdelmaseih R, Ashraf B, Abdelmasih R, Dunn S, Nasser H. Southern Tick-Associated Rash Illness: Florida’s Lyme Disease Variant. Cureus. 2021;13(5):e15306.
Dr. Daniel Cameron, MD, MPH
Lyme disease clinician with over 30 years of experience and past president of ILADS.
Symptoms • Testing • Coinfections • Recovery • Pediatric • Prevention


Emerging? I had multiple tick bites as a child during summer trips to Kentucky, in the early to mid 1970s.
I has taken a while for doctors and researchers to document ticks and tick borne diseases in new areas. Until someone writes it up, the typical answer might be we don’t have tick or we don’t have tick borne diseases in this area.
I have been ill since the spring of 1987 . I lived in a wooded area near a lake . I saw several Possums and Raccoons when I lived there . I had not lived there long and I was clearing brush and taking it into the woods . When I finished and was cleaning up . I found a Tick embedded in my left arm . I removed it with tweezers and flushed it .It wasn’t long before subtle changes began .Visual problems ,fatique and and a strange sensation in my left foot and left arm . Several months later I was diagnosed with Hemianopsia . I started having memory problems .Nobody seemed to know what was wrong . It wasn’t until 1999 and my mother was watching a show about Lyme Disease and she called me to tell me how the rash shown on the show looked the same as the one I developed after the Tick bite .I contacted a Infectious disease Doctor and he did treat me with iv antibiotics . I did get better after being bed ridden and having to use a walker while undergoing